By: Dr. Mike Caisse DPT
We are very lucky to be involved in such a well-connected community as Crossfit. In my opinion, we have access to some of the most intelligent, practical and well-read professionals of their respective fields in the world. Think about it… if we want to know more about nutrition, we have Dr Barry Sears. If we want to know how to run, we have Brian MacKenzie. If we want to know about gymnastics, we have Carl Paoli. Power lifting, Jesse Burdick. Oly lifting, Mike Burgener. And lastly, however, most importantly, if we want to know how to move and how to reach our genetic potential we have our beloved leader Kelly Starrett- MWOD Pro; and locally in San Diego of course, Movement-Rx.
Without optimal joint mobility, tissue elasticity and malleability none of us will ever reach or know our genetic potential. In fact, we will continue to fail over and over again to leverage our true physical capacities and most of us will sustain multiple injuries while trying. Most of our best athletes will ultimately fail to ever see their full potential because they do not understand the benefits of unlocking their bodies. Kstar once said that he’s only seen perhaps one or two of his elite athletes reach close to 90% of what they are capable of. This statistic is simply sad and disappointing, because we have the resources available to reach everyone, yet most of us are not leveraging this information. An example you probably are familiar with is Kobe Bryant and his Achilles tendon rupture. This injury was completely preventable and likely happened as a result of this athlete’s lack of knowledge regarding a combination of things including the importance of mobility and suppleness of the soft tissues and joints.
I am a doctor of physiotherapy, as is my colleague Dr. Theresa Larson (creator of Movement-Rx), and we see athletes everyday ranging from those who are devoted to training and competing in the Crossfit games to those who are working professionals who may sit at a desk for forty hours a week. Something that might be surprising but true is both of these aforementioned cohorts of people on average cannot even reach a neutral/normal joint position at the hip or ankle. And they are likely lacking 50% or more of their available range of motion in these joints.
What does it mean…?
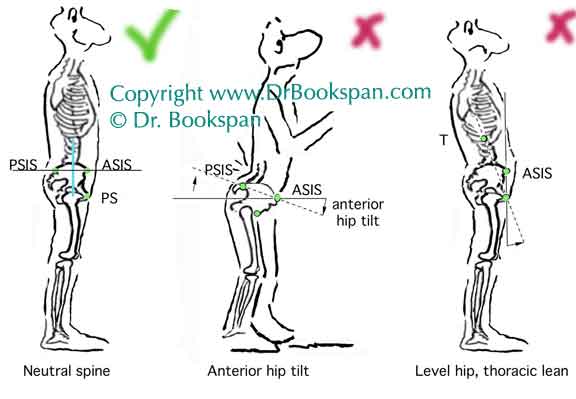
Hip Extension
Consider this, a human needs about 20 degrees of hip extension range of motion in order to move normally. To test yourself, try the following:
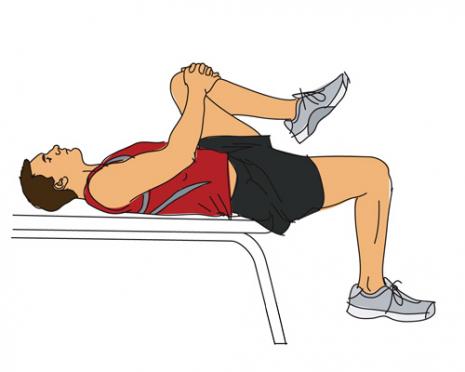
TEST POSITION. Lay on your back on the edge of a table (a bed or sofa will do) with thighs and legs hanging off so that the lower back and buttocks are just supported, knees relaxed
TEST. Pull your left knee toward your chest until the lower back is flattened against the table. The right thigh should hang below the level of the table about 20–30 degrees. Then switch legs and repeat the test.
The average range of motion for the leg hanging off the table is 20 degrees. The tissues in question are the hip flexors, Psoas major, psoas minor, iliacus, and rectus femoris.
Ankle Dorsiflexion
Also, we humans need 20 degrees of ankle dorsiflexion range of motion to perform basic movements that a two year old can do, like squatting. To test yourself, do the following:
TEST POSITION. Lay on your back with your feet flat against the wall (body perpendicular to
the wall).
TEST. Keep the heel in contact with the wall while attempting to pull the balls of your feet and toes away from wall. There should be a space of 1–2 inches between the ball of foot and the wall. Bear in mind that this test primarily emphasizes the gastrocnemius (calf muscle), while the alternative test below is more indicative of restrictions in the soleus, the other plantar flexors, and/or the ankle joint itself. Test both sides.
ALTERNATIVE TEST. Stand facing a wall with the toes roughly 2–3 inches from the wall. Attempt to bend the knees and touch them to the wall while keeping the heels on the floor. If the knee(s) touch, move backward in increments of about half an inch until the point at which the knees can no longer touch the wall. At the last point in which the knee(s) can still touch the wall, the distance between the toes and the wall should be about 3 inches. An inability to touch the wall is a significant restriction, especially if occurring on one side only. As this alternative test is performed in full weight bearing, there may be considerably more than the 20 degrees of dorsiflexion suggested above. The tissues in question are the foot, ankle, toe flexors, calf, Achilles, ankle and foot flexor muscles.
If we cannot get our bodies into these basic positions, then we certainly cannot expect to run, jump, press, squat, etc. without pain and eventually tissue failure and serious pathology.
It is our mission and personal agenda at Movement-Rx to teach and spread the message to everyone about taking responsibility for your bodies and performing the basic maintenance required in order to live a long and active life without pain. The information is here and all it takes is fifteen minutes of your time each day to improve your movement. There is no reason to be held hostage from achieving your goals due to a mobility issue.
If you want additional help in improving your performance, durability, and recovery, don’t limit yourself to your own knowledge and come see someone who can help you sort it out.
Sources:
Improve the sliding/gliding surfaces of the posterior structures of the lower leg (Bone Saw):
Do you think quarterback Mark Sanchez or defense tackle Kenrick Ellis have quality recovery and repair tactics post football practice and games. Besides being injured right now they both still have to have a game plan to help their tissues repair to be able to play and compete at such a high level.
Athletes (yes YOU!), HOW do you help your tissues repair after strenuous workouts or activities?
There are several key important components of tissue repair, including nutrition, sleep, and positioning. Today’s posting, however, is focused on repair time and the physiological inflammatory response of your tissues post exercise and how you can help speed up that process with some simple modalities.
It is common to have our bones, muscles, joints, tendons, and ligaments stressed in workouts- it helps us grow, get stronger, and continuously perform at higher and higher levels. Remember Wolff’s Law? This ‘juice’, or inflammation, that our body releases when we stress is a natural process. You probably already know how long it takes your body to repair after longer bike rides, flag football games, or met-con workouts versus shorter more intense workouts. Healthy tissue inflammation may only last a few hours; for an actual injury like both Sanchez and Ellis are dealing with swelling can last 24-48 hours to 2 weeks before it becomes chronic.
Getting nerdy with it again folks. Think of inflammation like troops deploying to a war zone. Your white blood cells are the troops and the damaged or strained tissue is the battlefield. Initially there is a neural reflex to cellular injury that causes vasoconstriction right away, then following this short period there is a vaso-dilation or opening up of vessels to allow blood to flow to the wound. This increase of the troops ammunition such as blood flow brings nutrients, oxygen, and phagocytes cells to the area that needs repair to help it heal .
Mission accomplishment in the above description of inflammation is that you flush the “juice” to the lymph system which is an open highway of helping the body eliminate waste quickly!
Legit Repair Tactics:
Compression- using a band of some sort (Vodoo band by MobilityWOD)
Elevation- I do not mean go to 18,000 feet, rather raise the limb and let the “juice” flow towards the lymph nodes located at major highways of the body such as the groin, armpit, and abdomen.
Heat– used by the Chinese for MANY years. Heat can be applied prior to and following workouts as long as there is no acute (24-48 hours to up to 2 weeks) injuries incurred. Please note that heat is contraindicated or have adverse effects with acute injuries. Heat causes capillaries (small blood vessels) to widen which is not needed if there is already inflammation in the tissue. If the injury is chronic (3-4 weeks to months/years), the need for blood flow and opening of that capillary network is important. In times of acute inflammation following an injury or even workout, simple compression and elevation is MOST useful.
Marc ProTM Device (MPD) – Helps with electromyostimlation (EMS). The MPD was designed to stimulate an ultra low frequency, low tension, non-tetanizing (continuous contraction of muscle tissue), and non-fatiguing contraction. It helps with the healing in the tissues by pumping arterial blood, fresh with “the troops or repair team” of fluids or inflammation, into the muscle and into capillary beds. This ammunition of fresh, oxygenated blood forces venous blood return and lymphatic draining, which carries all the metabolic waste products and damage away from the muscle.
The Enemy to natural tissue repair or What NOT to do:
Use NSAID’s- Non-Steriodal Anti-Iflammatories such as ibuprofen or motrin will help with your pain, but the reason the inflammation is occurring will not be fixed. It merely covers up the problem.
ICING- also just masks the problem and slows down the inflammation and further congests tissues that are working to drain into the lymphatic system. Icing can back up the lymphatic system which alone can cause problems with allowing tissues to heal in a normal period of time! http://www.mobilitywod.com/2013/07/community-video-peoples-weve-got-to-stop-icing-a-year-later
Supps- Take a bunch of supplements you are not educated about
Final Note: Thanks to the Resiliency Project, for every 4 Marc Pro’s purchased using the code KSTAR, 1 Marc Pro is donated to a veteran, active duty, or wounded warrior. If you want to learn more about the science behind the Mar Pro Unit: http://marcpro.com/new/the-science-behind-the-marc-pro
1. Athletic Lab. Inflammation Friend or Fo. Available at: http://athleticlab.com/blog/comments/inflammation-friend-or-foe/. Accessibility verified 4 Sept 2013
2. Hertling D, and Kessler RM. Management of Common Musculoskeletal Disorders; Physical Therapy Principles and Methods 4th Edition. Pennsylvania. Lippincott Williams and Wilkins. 2006
3.Cantu RI, Grodin AJ, Stanborough RW. Myofascial Manipulation: Theory and Clinical Application. Pro-ed. Texas. 2012
Lab #3 took place at Imperium CrossFit in Houston, Texas after the Just Roll With It Boot Camp Seminar. Dr. Larson worked with a Veteran and adaptive athlete named Tim Brumley (see video) who had recently hurt his lower back after performing the Memorial Day Warrior WODs and some heavy
This Lab will focus on Acute Low Back Pain and what to do about it!!
So…have you ever bent over to pick up your kid, dead lift, front squat, or snatch with poor form and or too much weight? Have you ever tried to pull a massive object like a boulder out of your driveway (hmm… my dad), carry a guy on your shoulders who is 2 X your weight (hmm…ME), and or pick up your baby after having a C-section and feel your back give out? Perhaps all you wanted to do was curl up in a ball and cry?
Do you have an athletic trainer who stalks you or is like your body guard? No? Really…why not! Just kidding, neither do I!
You are not alone! Millions of individuals in the United States suffer from acute low back pain for various reasons every year. Roughly $100 billion is spent every year on acute (7-14 days post injury) low back pain injuries according to the Journal of the American Osteopathic Association. [1] Chronic (3-4 weeks and up to 6 months post immediate injury) injuries are a whole different ball game and are also up there in terms of the billions of dollars spent in our health care system. These chronic conditions usually occur when the reason for the acute condition was not taken care of immediately!
These acute low back pain symptoms can range from spasms, burning pain down the leg, a centralized pain in the low back and/or butt region, or aching pain at the base of the spine. The pain may feel like a hot spot or like none of the muscles in your back are working. We all can call our primary care physician and get the top ten list of what medicine to take for the pain – naproxen, ibuprofen, even Vitamin M (military term for Motrin). But what can you do aside from ingesting pills to help alleviate the immediate symptoms that sometimes take you out of the game and literally lie you flat on your back with disbelief? Of course there are positions and lifting techniques to master, but for this short period of time, when you feel like you are in the twilight zone or the pain cave, let’s get you moving correctly!
As a sports medicine and performance-focused doctor of physical therapy, if you were my client -OR if I were still in the Marines and you were in my platoon or company – I would work to rectify the situation with proper movement, regardless of the issue. Vitamin M (Motrin) would be out of the question and we would seek to relieve the immediate symptoms with how you position yourself. Let me be clear that we are NOT taking into account any central nervous system damage, other traumas, or diseases such as ankylosing sponydyolysis, spinal osteoblastomas, osteoporosis, osteonecrosis etc. Rather we are talking about musculoskeletal injuries such as vertebral disc herniations, bulges, facet joint dysfunction, spondylolysis, sprains in the ligaments, or strains in the muscle supporting the spine. These injuries happen, and your doctor, physical therapist, chiropractor, coach, mommy or daddy may not be there or know how to coach you through what to do next, so here it goes!
Keep in mind all these techniques are to help get you back to moving correctly so you can function. It is merely a band-aid. The main thing to address is WHY this did happen in the first place. Those reasons are overuse, poor form, too much weight, or all of the above!
BACK SPASMS
If you have been having low back spasms for a few days from an overstressed muscle, sacroiliac joint dysfunction (a literal pain in the butt and your hips feel off), possible vertebral disc issue (the jelly doughnut between each spinal segment), or from a number of other symptoms, then check out the following video. Note: If your back “spasms” become debilitating or start radiating down your leg, or you feel numbness and tingling, please consult your primary health care professional to help you with a condition that might be more serious that you think.
Beyond what’s in the video, help the tissues of the back relax by applying heat in the form of a pad or a soak in a hot tub or bath. The strain-counter-strain is a good technique that can help alleviate muscles that are having spasm episodes or have a knotted feeling, but I am not demonstrating this in the video.
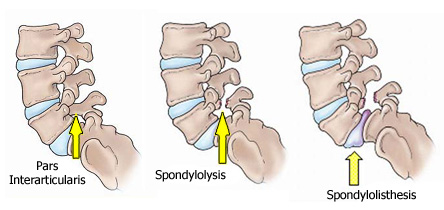
SPONDYLOLYSIS
(taken from orthoinfo@aaos.org)
A spondylolysis is defect or fracture of the pars interarticularis on the lumbar spine (see picture above), which surprisingly does not always express symptomatically. This fracture can turn into a spondylolisthesis which is a slippage of the vertebral body forward and can implicate the spinal cord if not taken care of IMMEDIATELY! This slippage is usually where the symptoms come from and can range from a hot spot like feeling, or numbness and tingling and or an aura of instability in the low back when performing any lifts from the ground!
Spinal stability (otherwise known as core stability) is essential as well as any activity that will help improve dynamic strength. By spinal stability I mean hips, low back, and abdominal’s; they all attach to your spine in some shape or form.
Find a health care professional who can help give you the appropriate dosage of load of exercise and trunk work (core) for the condition you have. This condition can happen due to a tackle in a football game, coming off a layup, and or performing an Olympic Lift with an already excessive overextended posture. Usually this happens at the Lumbar level 5-Sacral level 1 vertebral segments.
The name of the game – SPINE-and CORE STABILITY! As stated in the Journal of American Academy of Orthopedic Surgeons, “Current evidence suggests that decreased core stability may predispose to injury and that appropriate training may reduce injury.[2]” Do not try, I repeat DO NOT try to self diagnose and treat. Spinal cord damage can occur with a condition like this, if not take seriously! Invest in an evaluation and treatment program.
SPRAINS, STRAINS, and the LUMBAR DISC
The third issue I am going to discuss is low back pain that comes on after you pull, push, or apply a load to your low back that freaks it out and makes you want to curl up in a ball. Whether I was a Marine Corps lieutenant or DPT evaluating you (I am both), I’d tell you to “GET UP AND STAND UP STRAIGHT!! “ Do not curl up in a ball, and do not go to bed crying into your pillow in a flexed position!
Sure you may have had something like this before but remember it being less aggressive or painful, and you attempt your best self diagnosis. You may be quite certain it is your psoas major, or a lumbar strain, or you just know you were lifting with piss-poor form. No matter the self-diagnosis, stand up and keep that spinal curve in check. Do not overextend, do not flex forward, just stand up and maintain a neutral spine. As Dr. Kelly Starrett mentions in all his mobility and movement seminars and in his new book, Becoming a Supple Leopard, squeeze your butt as if your life depended on it! Whether it is a disc herniation, a fracture, a sprain or strain, give the structures in the back of your spine a chance to approximate the tissues, disc, and ligament’s versus tear further!
Like I mentioned before, this article is for acute conditions that are following an immediate low back injury at the gym, at home, doing yard work….anywhere. Take the immediate steps to not hurt yourself further and get some professional help on HOW to fully heal and fix the reason WHY this happened in the first place!
In an upcoming lab I will talk about ways to improve spinal stability that will ultimately be your shield of protection throughout the rest of your life!!
[1]Crow TW, Willis DR; JOAOA: 2009; 109, 229-233. Available from: American Osteopathic Association. Accessed June 2013
[2]Wilson JD, Dougherty CP, et al. JOAAOS: 2005, 13: 316-325. Available from: American Academy of Orthopaedic Surgeons. Accessed June 2013.





 (taken from orthoinfo@aaos.org)
(taken from orthoinfo@aaos.org)